























Health Impact
Behavioural therapy alongside medical treatment produces significantly better outcomes than medication alone
Dr. Ekant Budhwani
Dr. Ekant Budhwani is a Gastroenterologist, Hepatologist & Advanced Therapeutic Endoscopist, trained at AIG Hospitals, Hyderabad, and holds an ESEGH (UK) certification. He currently practices at Oraya Clinics, Shankar Nagar and Acellus Hospital, Avanti Vihar, Raipur.
At Oraya Clinics, Shankar Nagar and Acellus Hospital, Avanti Vihar, we offer a comprehensive, end-to-end gastroenterology and hepatology service designed to bring advanced care to Raipur and Central India.
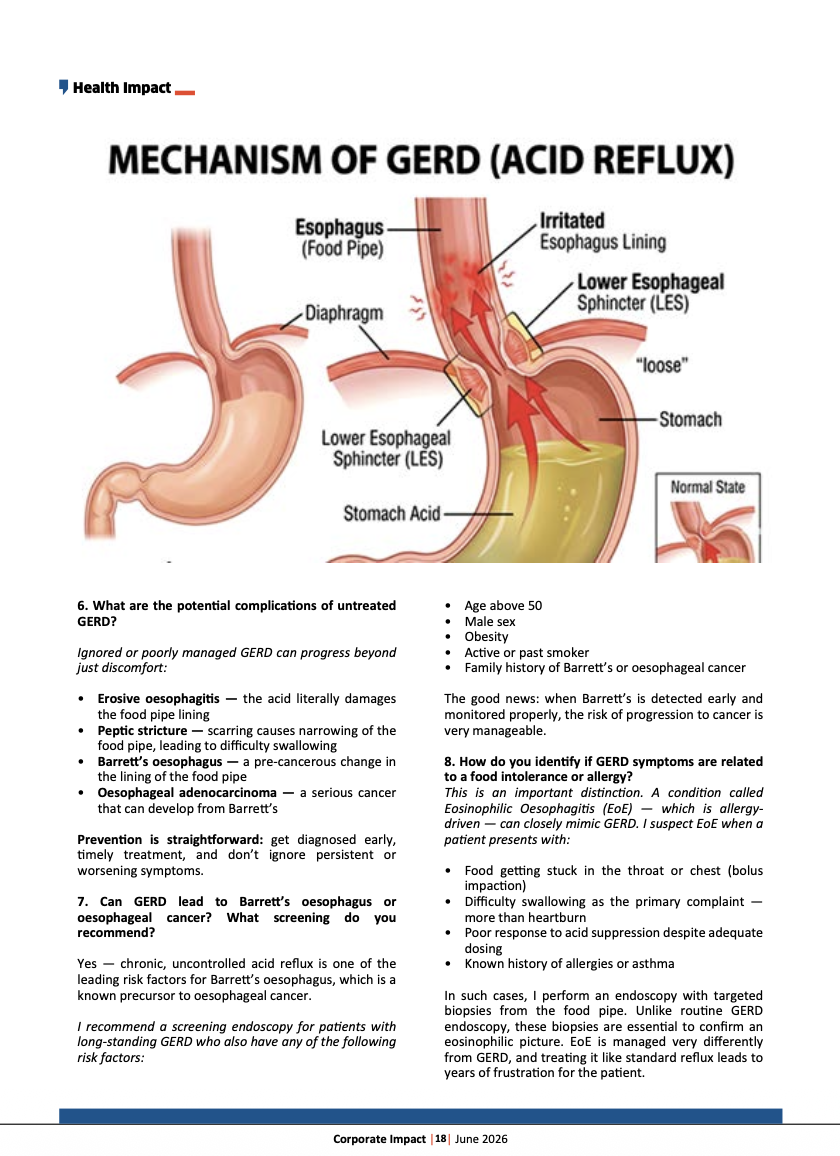
1. What are the primary factors that contribute to the development of GERD, and how do they affect the lower esophageal sphincter?
GERD occurs when the valve between the food pipe and stomach — the lower esophageal sphincter (LES) — stops working properly, allowing acid to flow back upward.
The main contributing factors are:
- Hiatal hernia — the most common anatomical cause; it physically weakens the LES
- Obesity — increases pressure within the abdomen, forcing acid upward
- Smoking — directly relaxes the LES, worsening reflux
- Certain medications — calcium channel blockers, nitrates, and some pain relievers can reduce LES tone
- Pregnancy — hormonal changes combined with increased abdominal pressure
- Dietary habits — large, fatty, or late-night meals trigger excessive LES relaxation
When the LES weakens or relaxes at the wrong time, it loses its function as a one-way valve — and acid reflux follows.
2. How do you diagnose GERD, and what tests do you recommend?
While GERD is often diagnosed clinically via typical symptoms and medication response, objective testing is vital before starting long-term therapy or considering procedures.
- Upper Endoscopy: The main test to check your food pipe for damage like ulcers or Barrett’s esophagus. It is best done while off acid medications.
- Acid (pH) Monitoring: Measures acid in your food pipe over 1 to 4 days. It is the best test if an endoscopy is normal but symptoms continue.
- Manometry: Tests your food pipe’s muscle function to rule out other swallowing problems that mimic GERD.
- Blood Tests & Imaging: Used to rule out other conditions if your symptoms are unusual.
I follow evidence-based diagnostic protocols, ensuring each patient gets a precise diagnosis rather than an assumed one.
3. What lifestyle modifications do you suggest for GERD?
Simple, consistent changes can dramatically reduce symptoms:
- Lose weight — even modest weight loss reduces reflux significantly
- Stop smoking — one of the most impactful changes you can make
- Elevate the head of your bed — gravity works in your favour at night
- No meals within 3 hours of bedtime
- Eat smaller portions — a full stomach increases pressure on the LES
These four or five steps, done consistently, often reduce the need for medication.
4. Are there specific dietary restrictions for GERD?
Honestly, blanket dietary restrictions for everyone don’t hold up well in current evidence. Rather than eliminating everything at once, I encourage patients to:
- Keep a symptom diary — identify your personal triggers (common ones include fried food, citrus, coffee, chocolate, carbonated drinks, and alcohol)
- Focus on portion control — how much you eat often matters more than what you eat
- Prioritise weight management — this has the strongest dietary evidence for GERD improvement
I tailor dietary advice to each patient’s specific triggers, lifestyle, and culture rather than giving a one-size-fits-all restriction list.
5. How do you approach GERD treatment?
Treatment is always individualised. My approach:
- First step — lifestyle modifications, always. No medication replaces them.
- Medications — for confirmed GERD with heartburn, Proton Pump Inhibitors (PPIs) are the first-line treatment. The goal is the lowest effective dose for the shortest necessary duration.
- Optimising therapy — if a patient doesn’t respond adequately, I investigate why: Is the diagnosis correct? Is the patient a rapid metaboliser of the medication? Are there co-existing conditions? Genetic testing for drug metabolism (CYP2C19) can sometimes guide us to a more effective PPI choice.
- Long-term planning — patients on PPIs for more than 6 months deserve a structured review and discussion about whether endoscopic or surgical options might offer a better long-term solution.
6. What are the potential complications of untreated GERD?
Ignored or poorly managed GERD can progress beyond just discomfort:
- Erosive oesophagitis — the acid literally damages the food pipe lining
- Peptic stricture — scarring causes narrowing of the food pipe, leading to difficulty swallowing
- Barrett’s oesophagus — a pre-cancerous change in the lining of the food pipe
- Oesophageal adenocarcinoma — a serious cancer that can develop from Barrett’s
Prevention is straightforward: get diagnosed early, timely treatment, and don’t ignore persistent or worsening symptoms.
7. Can GERD lead to Barrett’s oesophagus or oesophageal cancer? What screening do you recommend?
Yes — chronic, uncontrolled acid reflux is one of the leading risk factors for Barrett’s oesophagus, which is a known precursor to oesophageal cancer.
I recommend a screening endoscopy for patients with long-standing GERD who also have any of the following risk factors:
- Age above 50
- Male sex
- Obesity
- Active or past smoker
- Family history of Barrett’s or oesophageal cancer
The good news: when Barrett’s is detected early and monitored properly, the risk of progression to cancer is very manageable.
8. How do you identify if GERD symptoms are related to a food intolerance or allergy?
This is an important distinction. A condition called Eosinophilic Oesophagitis (EoE) — which is allergy-driven — can closely mimic GERD. I suspect EoE when a patient presents with:
- Food getting stuck in the throat or chest (bolus impaction)
- Difficulty swallowing as the primary complaint — more than heartburn
- Poor response to acid suppression despite adequate dosing
- Known history of allergies or asthma
In such cases, I perform an endoscopy with targeted biopsies from the food pipe. Unlike routine GERD endoscopy, these biopsies are essential to confirm an eosinophilic picture. EoE is managed very differently from GERD, and treating it like standard reflux leads to years of frustration for the patient.
9. What role does stress play in GERD, and what do you recommend?
While stress doesn’t directly cause GERD, the gut-brain connection makes you feel it more intensely. Anxiety lowers your pain tolerance, making your food pipe hypersensitive to even mild acid reflux.
Practically, I advise:
- Regular physical activity — even brisk walking helps
- Adequate, consistent sleep
- Mindfulness or breathing techniques for those with identifiable stress patterns
- For patients where gut-brain overlap is prominent — behavioural therapy alongside medical treatment produces significantly better outcomes than medication alone
10. When is surgery considered for GERD?
Surgery becomes a conversation when:
- Symptoms are confirmed but do not respond to optimised medical therapy
- The patient prefers a long-term solution over lifelong medication
- Regurgitation (the sensation of food or liquid coming back up) is the dominant symptom — this often responds poorly to medications alone
- Surgery: Minimally invasive procedures repair the weak valve between your food pipe and stomach, offering quick recovery.
- Incisionless Options: For smaller defects, endoscopic (no-cut) procedures are a perfect middle ground between daily medications and surgery.
11. What are the latest gastro care facilities available at your centre?
At Oraya Clinics, Shankar Nagar and Acellus Hospital, Avanti Vihar, we offer a comprehensive, end-to-end gastroenterology and hepatology service designed to bring advanced care to Raipur and Central India.
Our facilities include:
- State-of-the-art diagnostic endoscopy — high-definition upper GI scopy, colonoscopy, and therapeutic procedures
- Advanced therapeutic endoscopy — including procedures for early GI cancers, strictures, bleeds, and complex biliary conditions
- Complete liver disease management — from fatty liver and hepatitis to cirrhosis and liver function evaluation
- pH-impedance and manometry-based GERD workup — for patients who need objective, precise diagnosis beyond symptom assessment
- Personalised consultation and follow-up — with evidence-based, guideline-aligned treatment for every patient
